


 Sign Out
Sign Out
It is rapidly bactericidal and possesses the safety profile of a penicillin.
The prevalence of acquired resistance is geographically and time dependent and for select species may be very high. Local information on resistance is durable, particularly when treating severe infections. (See Table 1.)
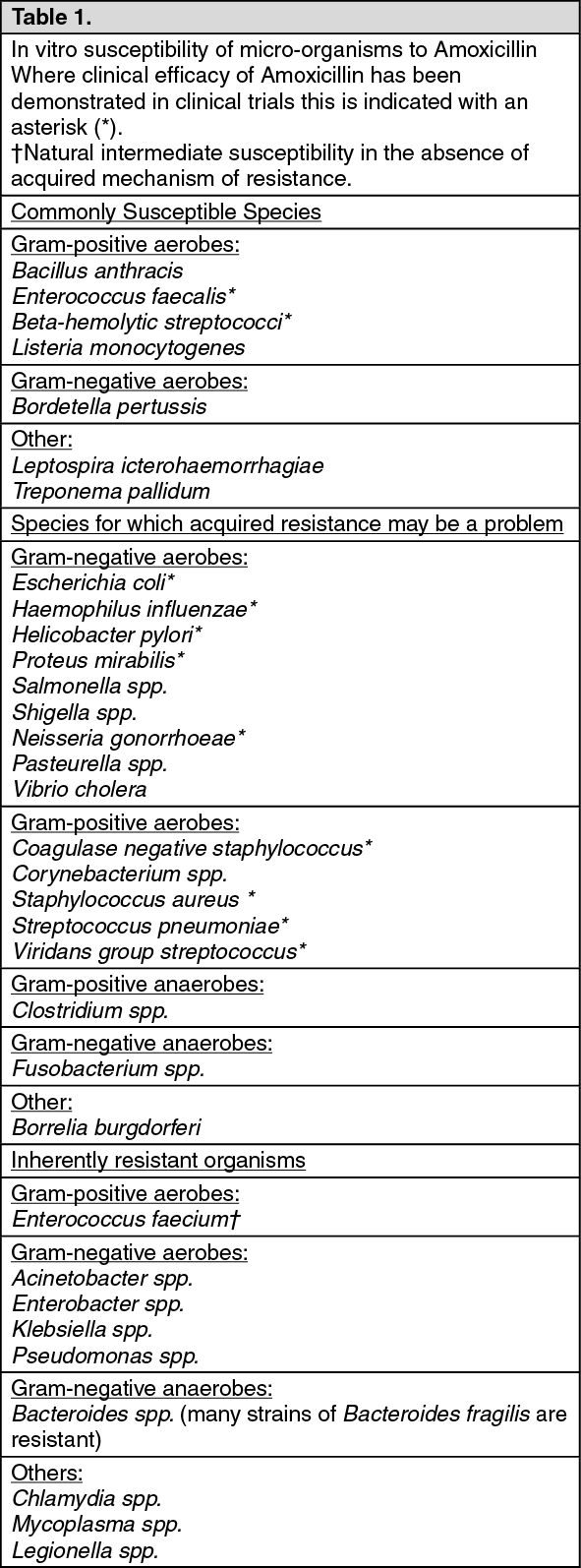 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Amoxicillin is well absorbed. Oral administration, usually at convenient three times a day dosage, produces high serum levels independent of the time at which food is taken. Amoxicillin gives good penetration into bronchial secretions and high urinary concentrations of unchanged antibiotic.
Amoxicillin is not highly protein bound; approximately 18% of total plasma drug content is bound to protein. Amoxicillin diffuses readily into most body tissues and fluids, with the exception of the brain and spinal fluid. Inflammation generally increases the permeability of the meninges to penicillins and this may apply to Amoxicillin.
The major route of elimination for Amoxicillin is via the kidney. Approximately 60 to 70% of amoxicillin is excreted unchanged in urine during the first six hours after administration of a standard dose. The elimination half-life is approximately one hour. Amoxicillin is also partly excreted in the urine as the inactive penicilloic acid in quantities equivalent to 10 to 25% of the initial dose.
Concurrent administration of probenecid delays Amoxicillin excretion.
Small amounts of the drug are also excreted in faeces and bile.